Bilateral sudden sensorineural hearing loss and chronic venous cerebrospinal insufficiency.
Bilateral sudden sensorineural hearing loss and chronic venous cerebrospinal insufficiency: a case report
D Alpini*, PM Bavera*, F Di Berardino†, S Barozzi† and A Cesarani†‡
*Scientific Institute S.Maria Nascente, Don C. Gnocchi Foundation; †Dipartimento di Scienze Chirurgiche
Specialistiche, Universita` degli Studi di Milano; ‡Audiology Unit, Fondazione IRCCS Ca’ Granda Ospedale
Maggiore Policlinico, Milan, Italy
Abstract
Objectives: We report a case of bilateral sudden sensorineural hearing loss (SSHL) in a patient suffering from chronic venous cerebrospinal insufficiency (CCSVI). Methods: Audiometric testing confirmed bilateral sensorineural hearing loss with hypoexcitability to caloric stimulation on the left side and echo-colour Doppler examination showed abnormal cerebral venous deficiency.
Results: The patient’s condition improved after 15 days following medical treatment.
Conclusions: CCSVI may explain the anatomical background which provides a predisposing factor for SSHL although further studies are needed to verify whether this observation is casual or coincidental.
Introduction
Sudden sensorineural hearing loss (SSHL) is defined as a sensorineural hearing loss of 30 dB or greater over at least three contiguous audiometric frequencies occurring within a 72-hour period.1
Various aetiologies have been proposed to explain SSHL including vascular mechanisms (microembolism, haemorrhage and thrombosis), inflammation, meningitis, syphilis, HIV infection, autoimmune inner ear disease, ototoxic drugs, tumours, traumatic and idiopathic mechanisms.2 SSHL has also been associated with vertebro basilar insufficency.
3–10 However, for the majority of patients an aetiological factor is not identified. The results of SSHL treatment are still largely unpredictable; a huge variability in responses has been reported ranging from no response to total recovery.(11)
However, the latest reports comparing different therapies have shown a pure-tone threshold (PTA) improvement of approximately 30 dB in responders with an initial PTA of 50–60 dB.12 Chronic venous cerebrospinal insufficiency (CCSVI) was initially described as being strongly associated with multiple sclerosis (MS).13 It is a syndrome characterized by stenosis of the internal jugular veins (IJVs) and/or azygous vein with opening of collaterals and insufficient drainage.
14 – 16 We report a case of bilateral SSHL with vertigo, showing evidence of the CCSVI pattern but not associated with MS. To the best of the authors’ knowledge, this kind of association has never been reported.
Case report
In 2010, a 56-year-old woman came to our observation for an SSHL in the right ear associated with aspecific dizziness and lightheadedness. In 2003, without any previous history of hearing difficulties, the patient had experienced an episode of SSHL in the left ear. In both episodes, there was no prior history of temporal bone fracture, meningitis, autoimmune disease or exposure to ototoxic drugs.
General and neurological evaluations were normal; extensive blood tests including liver function tests, complete blood count, urea nitrogen, creatinine, erythrocyte sedimentation rate, circulating immune complex and serum electrolytes all gave normal results. Antinuclear antibody, rheumatoid factor, C reactive protein, HIV and Venereal Disease Research Laboratory tests were unremarkable as were clotting
tests. A transthoracic echocardiogramand an electrocardiogram showed no abnormalities.
Audiometric testing, performed on admission, showed sensorineural hearing loss with a PTA at 500–1000–2000 Hz at 55 dB with 90% speech discrimination
in the left ear and PTA 45 dB with 95% speech discrimination in the right ear. Stapedial reflex thresholds at multiple frequencies were normal on both sides.
Normal waveform responses were evoked bilaterally on brain stem auditory evoked potentials.
Electronystagmography showed hypoexcitability (more than 22% asymmetry in our laboratory) to caloric stimulation on the left side. There were no abnormalities in saccades, pursuit or optokinetic nystagmus. Magnetic resonance imaging of the
brain, including diffusion images, was normal for a subject of this age.
The echo-colour Doppler for assessing cerebral venous return, according to the protocol of Zamboni et al.,17 showed an abnormal cerebral venous deficiency. A type B pattern characterized by significant stenoses of both IJVs and of the proximal azygous was observed. (Figure 1) Abnormal reflux of the vertebral veins and bilateral stenosis of the brachiocefalic junction were also detected.
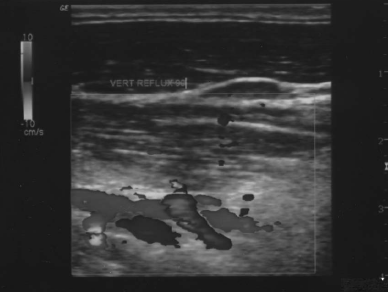
Figure 1 Reflux detected by the means of echo-colour Doppler at the level of the internal jugular vein
The problem we observed concerning the IJVs appeared to consist mainly of a malfunction of the valve leaflets that usually allow the correct outflow of the venous bloodstream and impede backstream. In both cases the leaflets appeared to have a reduced motility and, de facto, caused a stenosis of the vessel lumen. Secondly, the reflux of the vertebral vein system was quite evident, especially when the examination was performed in the upright position, since there was a poor outflow into the azygos venous system.
The patient was treated with systemic steroid, hyperbaric oxygen and platelet aggregation inhibitor 11 and an improvement of 35 dB of PTA was obtained in the right ear after 15 days. No modifications were observed in the left ear.
Discussion.
In 2007, Shim et al.18 presented a case of unilateral profound sensorineural hearing loss due to a venous malformation of the internal auditory canal. As expected, no malformations of the internal auditory canals were detected in our patient and therefore we had to focus on the possible effects of CCSVI on the outflow of the inner ear, that is completely drained by the vein of the cochlear aqueduct.
19 In fact, the common modiolar vein enters the bony channel immediately adjacent to the aqueduct to become the vein of the cochlear aqueduct which in turn drains via the inferior petrous sinus into the IJVs. Injury or occlusion of this vessel
would be particularly significant since it is widely believed to provide virtually the entire venous drainage of the cochlea.15,20 The cochlear aqueduct and the internal auditory canal communicate with the subarachnoidal space; in the guinea pig model, an occlusion of the veins of the cochlear aqueduct results in an increase of perilympatic endolymphatic pressure, a decrease of cochlear blood flow and
endolymphatic potential.
21Furthermore, since many of the venous vessels in the scala tympani have little or no bony covering and are essentially exposed to the perilymphatic space, the venous system is a route of entry for the cells participating in the inner ear inflammatory process.
22 Another interesting point is that the blood leaves the brain by using the back propulsion of the residual arterial pressure (vis a tergo), complemented by anterograde respiratory mechanisms (vis a fronte).1,2,4 – 7 The latter consist of the thoracic pump increased venous outflow during inspiration: the increase of negative thoracic pressure improves the aspiration of blood toward the right atrium. In addition to vis a tergo and vis a fronte, postural mechanisms play a fundamental role in ensuring a correct cerebral venous return. Several ultrasound studies of healthy volunteers have demonstrated that the pattern of cerebral venous drainage
changes, even under physiological conditions,
depending on the body position.
1,2,4 – 7 In the prone or supine position, the outflow through the IJVs is favoured, whereas passing to the upright position transfers most of the encephalic drainage to the vertebral veins.
1,4 – 7 On the basis of these considerations, it would be interesting to study the CCSVI in certain cases of bilateral SSHL following general anaesthesia for non-otological surgery involving the use of cardiopolmunary bypass of unknown origin23 since the CCSVI might explain the anatomical background which provides a predisposing factor for SSHL.
Further studies are needed to verify whether this observation is causal or coincidental.
References
1. Zivadinov R, Poloni GU, Marr K, et al. Decreased brain venous vasculature visibility on susceptibility-weighted
imaging venography in patients with multiple sclerosis is related to chronic cerebrospinal venous insufficiency.
BMC Neurol 2011;11:128
2. Zamboni P, Consorti G, Galeotti R, et al. Venous collateral circulation of the extracranial cerebrospinal outflow routes. Curr Neurovasc Res 2009;3:204–12
3. Zamboni P, Galeotti R, Menegatti E, et al. Chronic cerebrospinal venous insufficiency in patients with multiple sclerosis. J Neurol Neurosurg Psychiatry 2009;80:392–9
4. Zamboni P, Menegatti E, Galeotti R, et al. The value of cerebral Doppler venous haemodynamics in the assessment of multiple sclerosis. J Neurol Sci 2009;282:21–7
5. Koc¸ A, Sanisog˘lu O. Sudden sensorineural hearing loss:literature survey on recent studies. J Otolaryngol 2003;32:308–13. Review
6. Kuhn M, Heman-Ackah SE, Shaikh JA, Roehm PC. Sudden sensorineural hearing loss: a review of diagno-Q2 sis, treatment, and prognosis. Trends Amplif 2011 May [Epub ahead of print] PubMed PMID: 21606048
7. Stephan H,Wappenschmidt J, Kiefer H. Occlusion of the basilar artery. Neurosurg Rev 1981;4:41–52
8. Huang MH, Huang CC, Ryu SJ, et al. Sudden bilateral hearing impairment in vertebrobasilar occlusive disease. Stroke 1993;24:132–7
9. Deplanque D, Godefroy D, Guerouaou D, et al. Sudden bilateral deafness: lateral inferior pontine infarction. J Neurol Neurosurg Psychiatry 1998;64:817–8
10. Sunose H, Toshima M, Mitani S, et al. Sudden bilateral hearing loss and dizziness occurred with cerebellar infarction. Otolaryngol Head Neck Surg 2000;122:146–7
11. Conlin AE, Parnes LS. Treatment of sudden sensorineural hearing loss: I. A systematic review. Arch Otolaryngol Head Neck Surg 2007;133:573–81. Review
12. Rauch SD, Halpin CF, Antonelli PJ, et al. Oral vs intratympanic corticosteroid therapy for idiopathic sudden sensorineural hearing loss: a randomized trial. JAMA 2011;305:2071–9
13. Lee H, Whitman GT, Lim JG, et al. Bilateral sudden deafness as a prodrome of anterior inferior cerebellar artery infarction. Arch Neurol 2001;58:1287–9
14. Toyoda K, Hirano T, Kumai Y, et al. Bilateral deafness as a prodromal symptom of basilar artery occlusion. J Neurol Sci 2002;193:147–50
15. Buttner U, Ott M, Helmchen CH, et al. Bilateral loss of eighth nerve function as the only clinical sign of vertebrobasilar dolichoectasia. J Vestib Res 1995;5:47–51
16. Fetterman BL, Luxford WM, Saunders JE. Sudden bilateral sensorineural hearing loss. Laryngoscope 1996;106:1347–50
17. Zamboni P, Galeotti R. The chronic cerebrospinal venous insufficiency syndrome. Phlebology 2010;25:269–79
18. Shim HJ, Song DK, Lee SW, et al. A case of unilateral sensorineural hearing loss caused by a venous malformation of the internal auditory canal. Int J Pediatr Otorhinolaryngol 2007;71:1479–83. Epub 2007 Jun 22
19. Baloh RW. Dizziness, Hearing Loss, and Tinnitus. New York: Oxford, 1988:89–105
20. Schuknecht HF. Pathology of The Ear. 2nd edn. Philadelphia, PA: Lea and Febiger, 1993
21. Watanabe Y, Nakashima T, Yanagita N. Venous communications of the cochlea after acute occlusion of the vein of the cochlear aqueduct. Arch Otorhinolarygol 1988;245:340–43
22. Harris JP, Fukuda S, Keithley EM. Spiral modiolar vein: its importance in inner ear inflammation. Acta Otolaryngol 1990;110:357–65
23. Son HJ, Joh JH, Kim WJ, et al. Temporary bilateral sensorineural hearing loss following cardiopulmonary bypass – a case report. Korean J Anesthesiol 2011;61:162–5